Address
3633 Central Ave. Hot Springs, AR 71913
Phone
(501) 620-4449

Address
3633 Central Ave. Hot Springs, AR 71913
Phone
(501) 620-4449

Intradermal (ID) injection is a critical delivery method, targeting the immunologically rich dermal layer for vaccines, antigens, and aesthetic “skin booster” treatments. Despite its clinical benefits, the ID layer presents a strong mechanical barrier compared to other parenteral routes such as subcutaneous (SC) or intramuscular (IM). The skin’s unique histology requires clinicians to overcome significant viscoelastic resistance to successfully deposit fluid within the narrow 1–2 mm target zone of the papillary or reticular dermis.
The Dermis as a Mechanical Barrier
The biological resistance faced during ID delivery results directly from the following tissue properties:
To ensure accurate delivery, the clinician must apply physical forces that specifically counteract this biological resistance.
In medical device consulting, “injectability” describes how easily a formulation can be expelled through a delivery system into the target tissue. To improve device performance and clinician ergonomics, we use the Cilurzo Framework to break down the total force into sequential Newtonian components.
Primary Force Components
Analyzing the injection phase enables precise modification of the syringe-needle interface.
Operator Comfort Bands for Intradermal Injection
The following table categorizes the impact of Newtonian force on the clinician’s ability to perform a controlled ID injection:
| Force Band (N) | Interpretation |
| < 10 N | Very comfortable; uncommon in standard intradermal delivery. |
| 10–20 N | Comfortable; typical of highly dilute formulations. |
| 20–30 N | Moderately difficult; common for standard intradermal delivery. |
| 30–40 N | Difficult; significant operator fatigue and tremor risk. |
| > 40 N | Very difficult; warrants immediate hardware/formulation re-evaluation. |
Typical ID injections often reside in the “Difficult” band (30–40 N), necessitating a shift toward optimized hardware to ensure clinical safety.
The “Intradermal Paradox” illustrates a situation where the site provides significant immunological and aesthetic benefits but also exhibits the highest mechanical resistance among common parenteral routes. Data from Porcine Model Biomechanics—a dependable human tissue equivalent—measures the considerable effort needed for dermal penetration.
Average Plunger Force Requirements (Porcine Model)
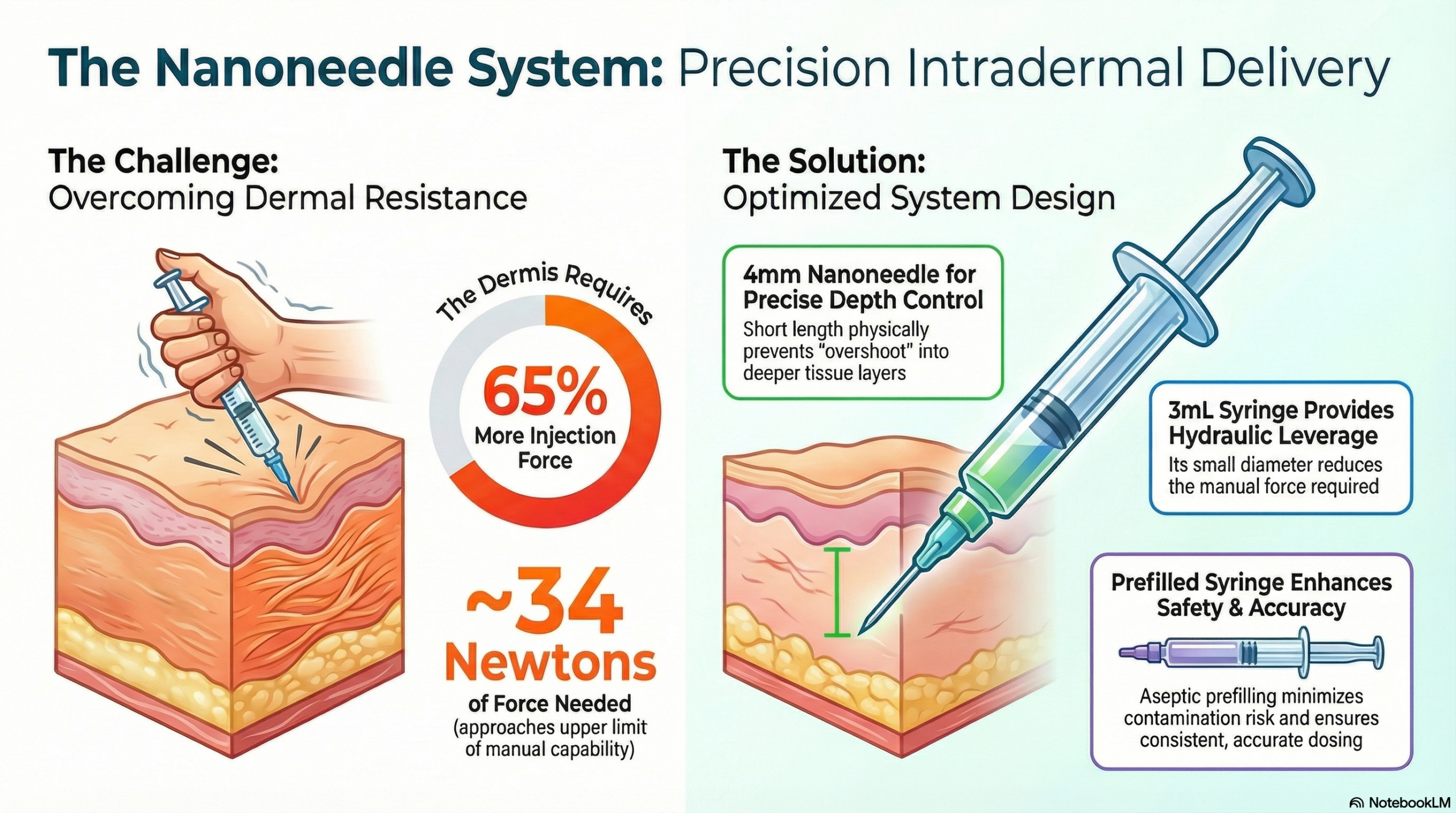
Empirical data shows a 65% increase in the force needed for ID injections compared to SC methods. This force difference is the main cause of clinical errors, especially injection variability and the risk of “overshoot.” In an overshoot situation, the high back-pressure causes the operator to lose control, leading to “subcutaneous failure” where the needle crosses the dermal-subcutaneous boundary and deposits the injectate into the fat layer. These high forces call for a complete re-evaluation of delivery hardware design.
The principle of “Hydraulic Advantage” is the most powerful tool in reducing injection resistance. Barrel diameter is the primary factor predicting the force an operator must exert on the plunger.
The mathematical relationship is governed by F = P·A, where force (F) is the product of pressure (P) and the surface area of the plunger (A). Since the area is proportional to the square of the diameter (A=π(d/2)^2), the force needed to produce a specific injection pressure increases exponentially rather than linearly as the syringe size expands.
Syringe Sizing Directives
Mechanical Advantage Comparison
| Syringe Size | Inner Diameter (ID) | Effort/Work Factor |
| 1-mL Syringe | 6.3 mm | 1x Work (Baseline Advantage) |
| 3-mL Syringe | 10.0 mm | 3x More Effort to overcome the same back-pressure |
Needle geometry and surface engineering are key factors in fluid dynamics and friction control. To ensure the bevel is correctly placed within the 1–2 mm dermal depth, clinicians should use a 15° entry angle.
The Thin-Wall Paradox
The “Nanoneedle” uses thin-wall technology to address the trade-off between patient comfort and fluid resistance. By reducing the thickness of the stainless-steel cannula, a 30G needle can have a wider internal lumen (effectively a 27G internal bore). According to Poiseuille’s Law, flow resistance is inversely proportional to the radius to the fourth power (1/r^4). This means a small increase in the internal bore causes an exponential decrease in the force needed for dense dermal entry.
Impact of Needle Length and Drag
Resistance to flow is also influenced by the Bernoulli Principle, where resistance is directly related to the length of the tube. A 4 mm needle reduces “frictional drag” along the inner cannula wall compared to a standard 13 mm needle. In addition to reducing force, the 4 mm length acts as a physical safety stop, preventing subcutaneous overshoot when used with the recommended 15° insertion angle.
Surface Engineering (Tribology)
Beyond geometry, surface engineering can modulate the needle-tissue interface. Advanced coatings such as Thin Film Metallic Glass (TFMG) utilize an amorphous atomic structure with a low Coefficient of Friction (0.05) and low Surface Free Energy (23.0 mN/m). TFMG coatings have been shown to reduce insertion force by approximately 66% and retraction force by approximately 72% compared to bare stainless steel, greatly enhancing the “glide” through non-compliant tissue.
The greatest reduction in glide force results from the synergy of optimized parameters. Using a small-diameter syringe combined with advanced Nanoneedle geometry can cut mechanical effort by 82%.
Synthesis Table: Effort Reduction
| Setup Type | Configuration | Resulting Force |
| Standard Setup | 3-mL Syringe + 13-mm Needle | 32.4 N (Near Failure Threshold) |
| Optimized Setup | 1-mL Syringe + 4-mm Nanoneedle | 5.7 N (82% Reduction in Effort) |
Engineering Best Practices
Switching from a qualitative to a quantitative, engineering-focused approach enables precise control of intradermal delivery. Using these biomechanical principles, clinicians can enhance safety, gain better control, and achieve consistent patient outcomes.